Incisional Hernia
Incisional Hernia | Hernia cicatricea | incisional hernia
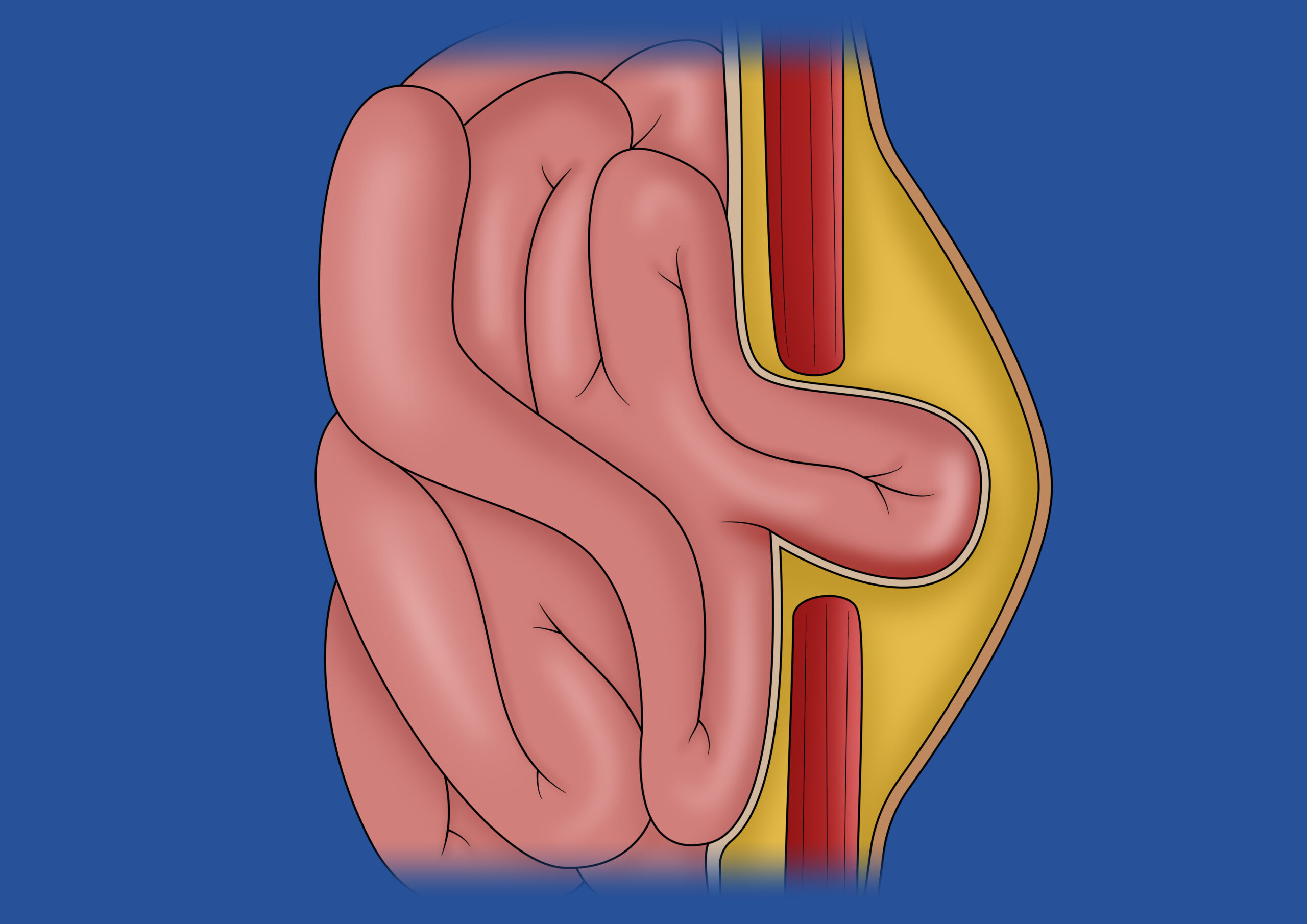
Incisional hernias are a common late complication of abdominal surgical procedures. The risks of developing incisional hernias are multifactorial, depending on the type of primary intervention and the method of abdominal wall closure. The incidence of incisional hernias after laparotomies is reported in the literature to be 10-20%.
Two-Column Text
- Chemical Component Separation with Botulinum Toxin (Botox)
Incisional hernias with a diameter exceeding 10 cm generally cannot be closed directly without tension. To facilitate abdominal wall closure and increase muscle extensibility, botulinum toxin (Botox) is injected preoperatively into the lateral abdominal muscles. This neurotoxic agent induces temporary muscle relaxation, which lasts approximately 2 to 5 months. The maximum effect occurs 3 to 4 weeks post-injection.
- Rives-Stoppa Sublay Technique (Operating time approx. 180 min)
In the sublay technique, a synthetic mesh is placed beneath the abdominal muscles through a skin incision. This method is particularly suitable for larger incisional hernias, as it provides stable reinforcement of the affected areas, offering a reliable and long-term solution.
- (e)MILOS or robot-assisted TARUP or (r)TEP Technique (Operating time from 120 min)
For larger incisional hernias, minimally invasive procedures are increasingly employed, such as the endoscopic-assisted MILOS technique or the robot-assisted TARUP and TEP methods. In these techniques, the synthetic mesh is positioned beneath the abdominal muscles. The operation is performed either laparoscopically or with the assistance of the DaVinci Xi System. The robotic variant allows for precise and gentle execution. The significant advantage of these procedures lies in their minimally invasive approach, which enables faster recovery and reduced postoperative burden for patients.
- Robot-assisted PeTEP technique (preperitoneal extended totally extraperitoneal) (surgery duration: approx. 120 min)
The rPeTEP technique is a modern, minimally invasive method for treating small to medium-sized abdominal wall defects. I prefer to use a so-called “bottom-up” approach from the lower abdomen, which allows for anatomical reconstruction of the abdominal wall while minimizing discomfort for the patient. A particular advantage of this technique lies in the cosmetic outcome: the incisions are located in the so-called bikini line and are therefore barely visible later on. In addition to the functional restoration of the abdominal wall, this also achieves a highly aesthetically pleasing result.
- Posterior Component Separation – (r)TAR Technique according to Novitzky (Operating time approx. 270 min)
Posterior component separation is performed either via an open incision or robotically assisted. This technique involves placing the synthetic mesh extensively over the lateral abdominal musculature, significantly reducing tension and expanding the mesh placement area. In the (r)TAR technique, the synthetic mesh is permanently positioned between the peritoneum and the abdominal muscles, specifically the rectus abdominis and transversus abdominis muscles, to ensure stable support for the affected areas. The extended compartment dissection facilitates the advancement of the posterior rectus sheath and enables midline (linea alba) reconstruction. This technique not only enhances abdominal wall stability but also substantially reduces the risk of recurrence.